EHRs can send records to hospitals, but when they arrive, much of the clinical data may live in unstructured documents, such as PDFs, or use codes the receiving system can't automatically interpret. That gap between being able to send data and being able to use it is the difference between foundational interoperability and semantic interoperability, and it's where most healthcare organizations get stuck. The Centers for Medicare & Medicaid Services Promoting Interoperability Programs are pushing eligible hospitals to close that gap, with Medicare payment adjustments tied to interoperability performance.
Understanding data interoperability standards in healthcare, the benefits of FHIR over HL7, and the real-world challenges of EHR interoperability will help you get ahead of the curve instead of scrambling to meet program deadlines.
TLDR:
EHR interoperability is the ability of different electronic health record systems to exchange patient data and help clinicians make use of it.
When EHR systems can't exchange data in a clinically meaningful way, the consequences can be severe: clinicians make decisions without complete information, patients repeat themselves at every appointment, redundant tests get ordered, and care coordination breaks down across transitions.
For value-based care organizations, interoperability is foundational. Without visibility into where patients receive care, managing population outcomes is nearly impossible.
HIMSS defines four levels of interoperability that apply across health systems, each building on the last.
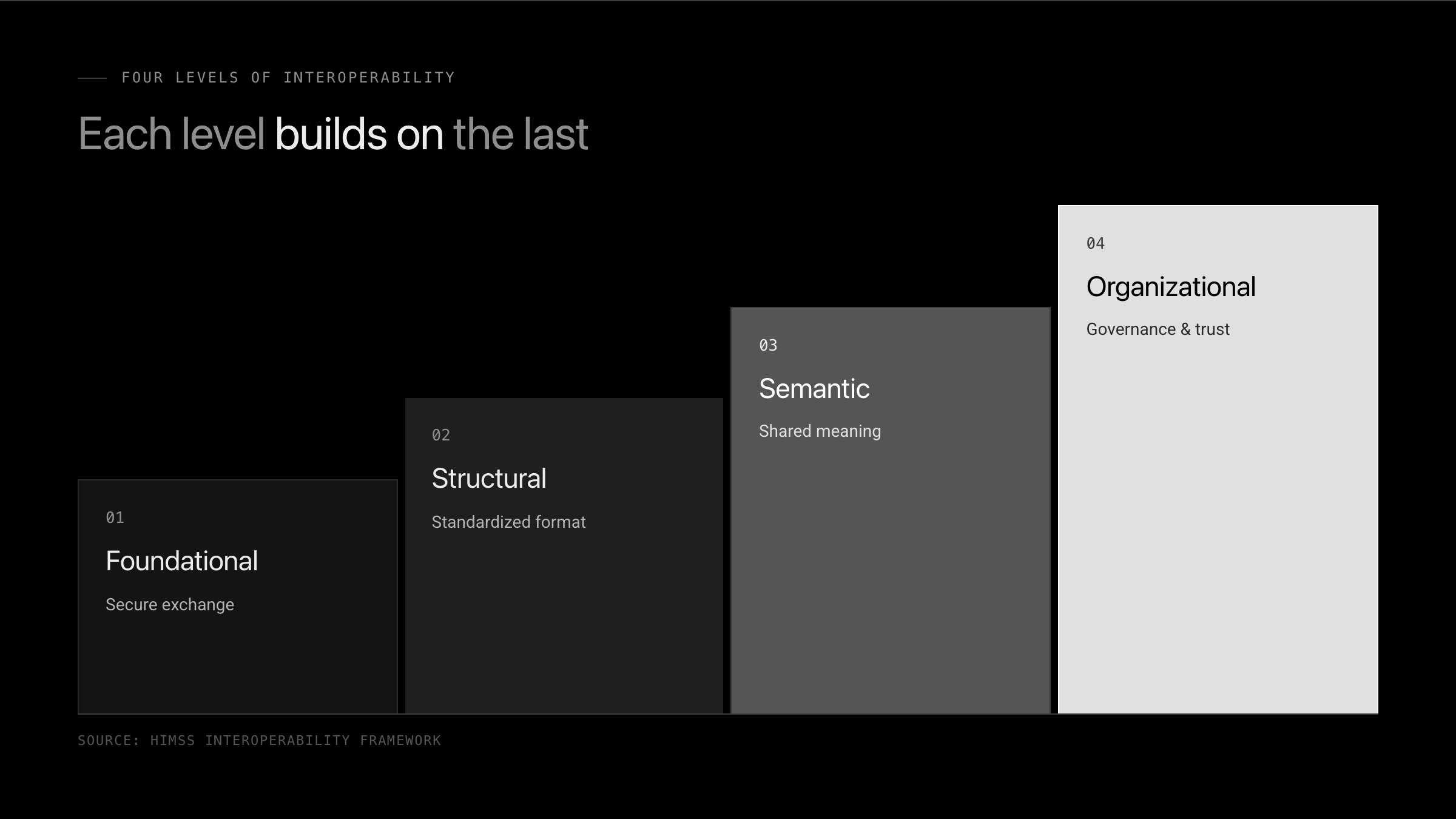
The most persistent EHR interoperability challenges occur at the semantic and organizational levels.
HL7 (Health Level Seven) and FHIR (Fast Healthcare Interoperability Resources) are the two standards that govern how health data moves between systems. HL7 v2 has been the backbone of clinical data exchange since the 1980s. FHIR, developed by HL7 International, is a modern interoperability standard that uses REST-based APIs to make health data more accessible to web and mobile applications.
FHIR organizes clinical information into discrete "resources" like Patient, Observation, and MedicationRequest, making it easier for developers to build integrations without deep healthcare IT expertise.
| Standard or Framework | Primary Purpose | Technical Approach | Current Requirement Status |
|---|---|---|---|
| HL7 v2 | Clinical data exchange messaging between hospital systems | Older messaging standards from the 1980s | Still widely used alongside growing FHIR adoption |
| FHIR R4 | Web-based health data exchange for modern applications | REST-based APIs organizing data into discrete resources like Patient and Observation | Required for certified health IT |
| USCDI V3 | Defines minimum data classes that certified health IT must exchange | Content layer specifying what data flows, including SDOH and care team information | Current USCDI standard for certified health IT |
| C-CDA | Structured clinical document exchange between EHR systems | XML-based documents with standardized formatting | Active but inconsistently implemented across vendors, causing semantic gaps |
USCDI defines the minimum set of data classes and elements that certified health IT products must be capable of exchanging. Version 1 set a baseline covering allergies, clinical notes, medications, and lab results. Version 3 expands considerably, adding social determinants of health, health insurance information, and care team member data. Under the ONC certification timeline, USCDI V3 replaced earlier versions for applicable certification criteria. For organizations building on FHIR, USCDI V3 defines what data needs to flow, making it the content layer to FHIR's technical structure.
That change matters beyond adding fields. SDOH (Social Determinants of Health) data affects care planning in ways a diagnosis code alone can't capture. Standardizing its exchange means systems can share context in addition to clinical facts.
The 21st Century Cures Act and CMS Promoting Interoperability Programs have reshaped how health systems share data. Providers must meet specific requirements or face Medicare payment penalties. The Promoting Interoperability Program evolved from the Meaningful Use program, shifting the emphasis from EHR adoption and basic use toward interoperability, patient access, and electronic data exchange. In 2025, requirements expanded the use of patient access APIs and electronic data exchange. Recent CMS interoperability requirements push healthcare organizations toward real, measurable interoperability instead of checkbox compliance.
Standards and regulations set the rules, but several real-world barriers make compliance harder than it looks on paper.
Closing the gap between where most organizations sit today and where semantic interoperability requires them to be takes progress on multiple fronts.
Process matters as much as the technology. Clinical staff need workflows that surface external data without adding steps, or adoption stalls regardless of what the integration layer can do.
FHIR-based APIs have become the standard mechanism for health data access and are required under ONC certification criteria for certified health IT.
These APIs let authorized applications retrieve patient records without proprietary data-sharing agreements slowing things down.
Standardized APIs lower the barrier for health tech developers building on top of EHR data, supporting everything from patient-facing apps to clinical decision support tools. When data follows a shared format, systems can exchange records without custom-built connectors for every integration.
When a clinician has a patient's complete history at the point of care, the downstream effects are concrete. Duplicate lab orders drop. Medication reconciliation becomes faster and more reliable. Allergies don't get missed because a previous provider's records weren't available.
Care coordination across settings is where the benefits compound most visibly. A primary care physician who can see an ED visit from last week, along with the discharge medications, can follow up before a readmission happens. Value-based care organizations depend on that cross-setting care event data to manage attributed populations and hit quality benchmarks tied to HEDIS and Medicare Stars measures. Without interoperability, those gaps stay invisible until they show up as costs or adverse events.
For patients, the benefit is simplicity: fewer repeated intake forms, fewer redundant imaging studies, and providers who actually know their history before the appointment starts.
Metriport gives healthcare organizations a single API to query and contribute patient records across major interoperability networks and frameworks, including CommonWell and Carequality.
Built on FHIR R4, it normalizes clinical data from interoperability networks into standardized resources into standardized resources so care teams get clean, structured records without manual reconciliation. Developers can go from sandbox to production quickly on Metriport's SOC 2 Type II certified platform, which simplifies document retrieval, data consolidation, and the complexities of healthcare interoperability.
Interoperability is not something you implement once and forget. Standards evolve, USCDI versions expand, and networks grow. Organizations that treat this as infrastructure instead of a project will adapt faster when requirements shift. The work is ongoing, but the returns compound when your systems can actually talk to each other without custom engineering every time.
EHR interoperability enables different electronic health record systems to exchange patient data and use it in a clinically meaningful way. It goes beyond just sending files. Systems must parse and interpret the data they receive so clinicians can act on a complete, usable patient record.
Interoperable EHRs help clinicians make better-informed decisions by providing access to a more complete patient record across care settings. They reduce manual record gathering, improve care coordination between providers, and give organizations a more comprehensive view of patient care. For value-based care organizations, interoperability also improves visibility into care delivered outside their own systems, supporting population health management and quality reporting.
The US lacks a national patient identifier, so matching relies on demographic information like name, date of birth, and address. Shared demographics, name changes, and moves all increase the risk of incorrect or duplicate matches. C-CDAs are implemented differently across EHR vendors, vocabulary gaps persist despite LOINC and SNOMED CT, and some vendors limit data portability to protect market position. Solutions include adopting FHIR R4, connecting through HIEs instead of building point-to-point integrations, investing in patient identity resolution, and testing interoperability continuously as vendors update their implementations.
The US lacks a national patient identifier, so matching relies on demographic information like name, date of birth, and address. Shared demographics, name changes, and moves all increase the risk of incorrect or duplicate matches. C-CDAs are implemented differently across EHR vendors, and vocabulary gaps persist despite standards like LOINC and SNOMED CT. Solutions include adopting FHIR R4, connecting through HIEs instead of building point-to-point integrations, investing in patient identity resolution, and testing interoperability continuously as vendors update their implementations.
FHIR is the better choice for modern health IT because it uses REST-based APIs that work with web and mobile applications, while HL7 v2 relies on older messaging standards. FHIR organizes clinical information into discrete resources like Patient and Observation, making it far easier for developers to build integrations without deep healthcare IT expertise. HL7 has been the backbone of clinical data exchange since the 1980s, but FHIR provides the technical foundation modern healthcare applications need.
The Promoting Interoperability Program is a CMS initiative that replaced Meaningful Use and requires providers to meet specific data exchange requirements or face Medicare payment penalties. As of 2025, requirements include patient access APIs and care coordination measures tied to FHIR standards, shifting focus from EHR adoption to actual data exchange.
Get the latest updates and blog posts from the Metriport team.



